Common adverse reactions observed in ≥2%, excluding hypoglycemia1


These adverse reactions, which exclude hypoglycemia, were not present at baseline, occurred more commonly on AFREZZA than placebo and/or comparator.1
What are the most common adverse reactions with AFREZZA?
The most common adverse reactions associated with AFREZZA are hypoglycemia, cough, and throat pain or irritation. In clinical trials, cough occurred in AFREZZA-treated patients with T1D and T2D at rates of 29% and 26%, respectively; in SC insulin comparators with T1D, 5%; and in placebo-treated patients with T2D, 20%.1 The majority of cough episodes were intermittent or single-defined events. Approximately 3% of patients discontinued AFREZZA due to cough in clinical trials.2
Cough was generally mild, and declined with use3
Incidence of cough in pooled safety population3

Pooled data from 13 phase 2/3 clinical studies in 5505 patients with T1D or T2D treated with AFREZZA, Technosphere inhalation powder without insulin (TP; placebo), or active-comparator treatment were analyzed for incidences of respiratory treatment-emergent adverse events. Study sample size reduced over time: from 3017 (AFREZZA) and 2198 (comparators) at Week 1 to 2563 (AFREZZA) and 2034 (comparators) by Week 12.2,3
Safety—lung function1
Monitor lung function with AFREZZA1


FEV1 test provided when patients start on AFREZZA
Request information about an FEV1 kit
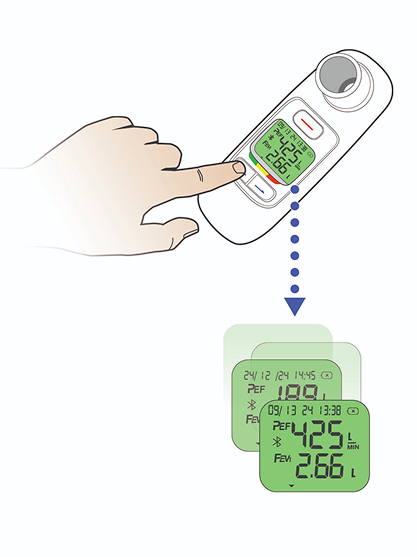
Conducting a FEV1 test7
Insert mouthpiece and switch device on

Instruct patient to exhale 3 times
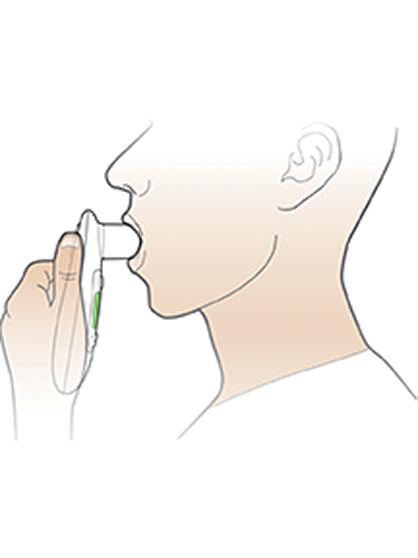
Record best FEV1 result
What pulmonary monitoring is required for all patients on AFREZZA?
Spirometry (FEV1) is required for all patients before initiating AFREZZA, at 6 months after starting therapy, and annually thereafter—even in the absence of pulmonary symptoms. AFREZZA causes a small but greater decline in FEV1 compared with comparators (mean difference, 40 mL over 2 years in clinical trials). In patients with a FEV1 decline of ≥20% from baseline, discontinuation should be considered. The 40-mL average difference represents approximately 1% of total lung capacity and differences were nonprogressive in trials lasting up to 2 years.1,4
FEV1, forced expiratory volume in 1 second; SC, subcutaneous; T1D, type 1 diabetes; T2D, type 2 diabetes; TP, Technosphere placebo.
References: 1. AFREZZA. Prescribing Information. MannKind Corporation; 2026. 2. McGill JB, Peters A, Buse JB, et al. Comprehensive pulmonary safety review of inhaled Technosphere® insulin in patients with diabetes mellitus. Clin Drug Investig. 2020;40(10):973-983. 3. Data on file (ISS). MannKind Corporation. 4. Oches M, O’Brodovich H. 5 – The structural and physiologic basis of respiratory disease, In: Kendig & Chernick’s Disorders of the Respiratory Tract in Children. 8 ed. W.B. Saunders; 2012:35-74. 5. Raskin P, Heller S, Honka M, et al. Pulmonary function over 2 years in diabetic patients treated with prandial inhaled Technosphere insulin or usual antidiabetes treatment: a randomized trial. Diabet Obes Metab. 2012;14(2):163-173. 6. Levin PA, Heinemann L, Boss A, Rosenblit PD. Impact of symptomatic upper respiratory tract infections on insulin absorption and action of Technosphere inhaled insulin. BMJ Open Diabetes Res Care. 2016;4(1):e000228. 7. Sonmol PEF. User manual. 2023.
© MannKind Corporation May 2026. US-AFR-2898